All I learnt about ANA
Do you like history ?
If No, You can Skip this part
ANA test started off as LE cell Phenomenon in Mayo clinic in 1948, demonstrated by Hargraves, Richmond and Morton. But this was insensitive and non-standardized.
1950:Fluorscein labeled antibodies were used to identify the tissue antigens in Boston by Coons and Kaplan.
1957:In Taplow, UK, Fluorescent labelled antibody technique was used to demonstrate that sera of LE cell positive patients contained antibodies that produce nuclear fluorescence on binding to nuclear antigen in human tissues.
1967: Rat liver sections were used to different patterns of staining such as homogenous, speckled, nucleolar by Beck in National institute of Medical Research in London.
1970s -80s : Use of Human cells to recognize various patterns in California by Dr. Tan in Scripp’s Clinic, California, USA.
What are HEp2 cell lines ?
HEp2 cells are Human epithelial cells, that originated from Human Laryngeal Carcinoma(HeLA cell contamination).
Why HEp-2 cell lines?
- They are grown in monolayers ensures better visibility
- Human origin ensures better specificity
- Larger nuclei
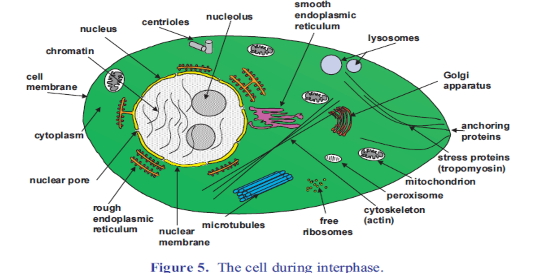
- Higher rate of cell division: Antigens produced during cell division(centromeres) are easily located. See the interphase of the cell division below.
- Cells at all stages of cell cycle.
But HEp2 IIF : is laborious, needs skilled technician, has interobserver variability. Different HEp2 Kit may lead to variability
- Not as sensitive for SSA/SSB/ myositis antibodies
ACR recommends using Hep2 cell lines for Indirect Immunofluorescence as gold standard for ANA testing. ANA by IIF (Indirect Immunofluorescence)
HEp 2 cell line interphase provides good substrate of Antigen for antibodies in sera to bind to to.
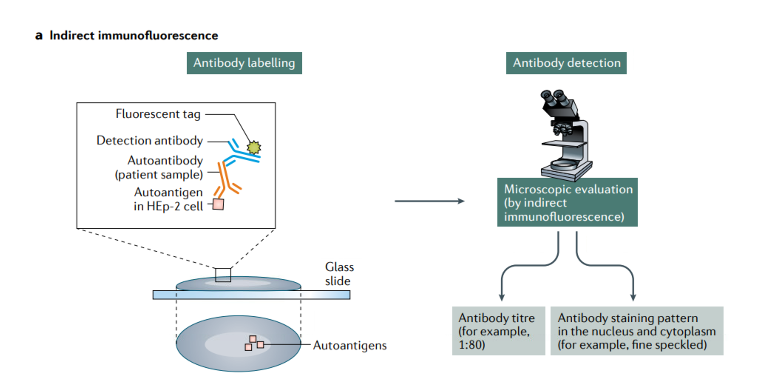
What is dilution or titer in ANA ?
When fluorescence is seen by performing above IIF method, the next step is to dilute the serum and see if the fluorescence still persist. If still does, continue to dilute until fluorescence disappears.
When equal part of diluting solution is added to the serum it is called 1:1 , and fluorescence persist, so we add another equal amount of diluting serum now the dilution is 1:2 . If dilution persists again, we add another equal amount of serum and so on.
The titer that is most helpful clinically is 1:80. Which means 1:80 was the last titer that the fluorescence was noted. On diluting further over 1:80, fluorescence disappeared.
Higher the titer , Higher the likelihood of autoimmune disease.
ACR/EULAR recommends at least 1:80 to consider a positive ANA. At 1:80, the sensitivity is 97.8%
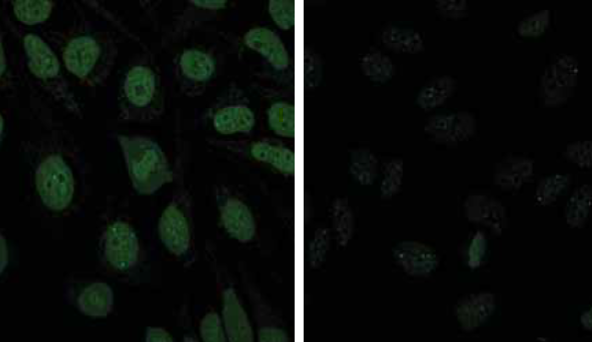
This is picture demonstrating, ANA positivity with lower dilution on left, and as you increase the dilution, you see decrease in fluorescence (decreasing titers).
Does Positive ANA means Lupus ?
No. ANA always needs to be interpreted with context of clinical features . Do not test ANA if your pretest probability is low.
For example: An elderly woman with fatigue, arthralgia without arthritis, you send ANA that is now positive 1:80 , what do you do?
Your pretest probability in this case is low. She doesn’t have arthritis, synovitis or rash or any other signs of SLE . Your post test probability is low as well. Patient develop antibodies as they go through life. Normal population can have ANA. In absence of clinical features, you don’t do anything. Hence , in the above scenario ANA testing was a waste of your resources, and creates unnecessary anxiety in patients.
Tan et al[1]
| ANA titers | Healthy Individuals |
| 1:40 | 31.7% |
| 1:80 | 13.3% |
| 1:160 | 5% |
| 1:320 | 3.3% |
Will patients with positive ANA develop symptoms?
Uncertain. ANA and SSA are the most common antibodies that have been detected a decade before onset of symptoms in a small Swedish study .[2]
Some Rheumatologist would err on the side of caution and monitor them yearly for symptoms.
Will patients with positive ANA develop symptoms?
Uncertain. ANA and SSA are the most common antibodies that have been detected a decade before onset of symptoms in a small Swedish study .[2] But Patients with SLE usually have positive ANA for few years before onset of the disease symptoms
Some Rheumatologist would err on the side of caution and monitor them yearly for symptoms.
Below is a time to event analysis from Arbuckle et al study. This is a famous study done on 130 veterans who were diagnosed with SLE, the investigators went back and tested their serum collected years (department of serum repository bank for veterans)before their diagnosis for SLE for autoantibodies and found anti smith and Anti RNP had closer temporal relationship between the development of antibody and onset of disease.Over 90 percent of patients who were ever positive for antinuclear, anti-Ro, anti-La, antiphospholipid, or anti–double-stranded DNA antibodies had a positive test long before the first clinical manifestation of SLE.
To read more about this study: Development of Autoantibodies before the Clinical Onset of Systemic Lupus Erythematosus | New England Journal of Medicine
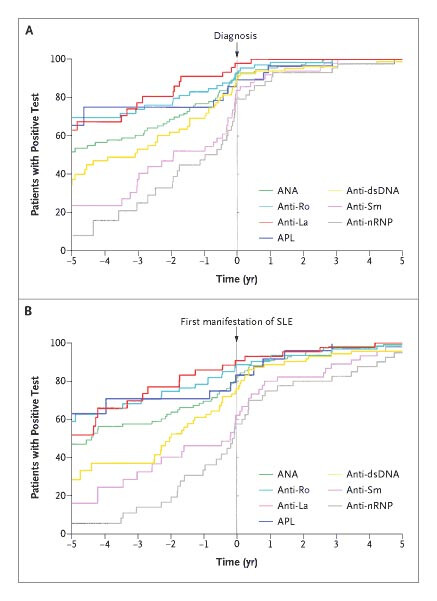
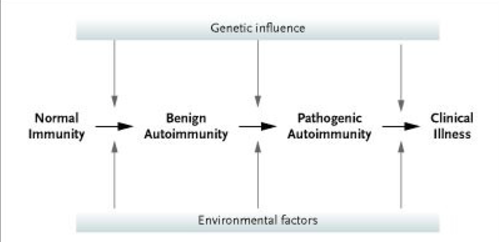
Aurbuckle et al., emphasized the concept of crescendo of autoimmunity. What that means is, there is a period of benign phase/ asymptomatic phase of autoimmunity before the disease onset, where there is accumulation of these various pathogenic antibodies. How I look at it is , when I see a smith and RNP positive in symptomatic patients, that alerts me to closely monitor these patients with symptoms, as these are more specific and start to appear more closer to the disease onset.
It is also important to looks for other causes for positive ANA, most common being malignancy and infection.
Most common non rheumatic conditions associated with positive ANA
- Thyroid disease : Graves, Hashimoto’s
- Primary Biliary Cholangitis
- Autoimmune hepatitis
- Infections: HIV, HBV, HCV, EBV, Tuberculosis, Endocarditis
- Malignancy: Lymphoproliferative
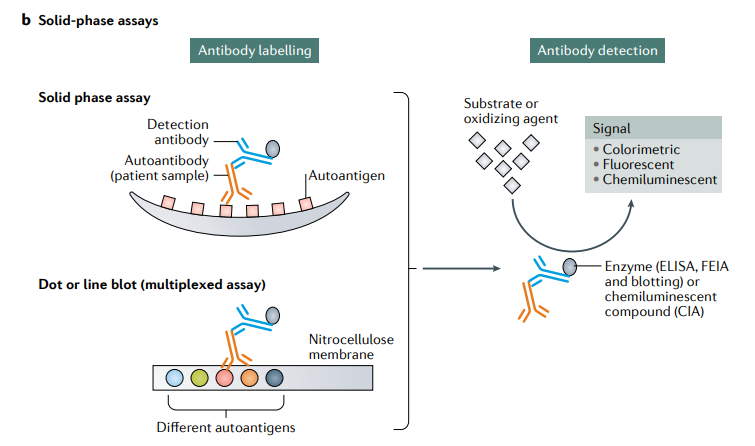
There are other methods to test ANA other than ANA by IIF on HEp 2 Cell lines. They are Solid Phase Assays.
| Hep2 IIF[3] | Solid Phase Assay |
| More sensitive for screening SLE and scleroderma | Not all antigen for scleroderma is used |
| Sjogrens Ab and JO1 can be missed | More sensitive for screening Sjogrens |
| Low sensitivity for IIM antibodies | Low sensitivity for For IIM Antibodies |
Solid Phase Immunoassay/ ELISA
- They are highly reproducible
- Cost effective
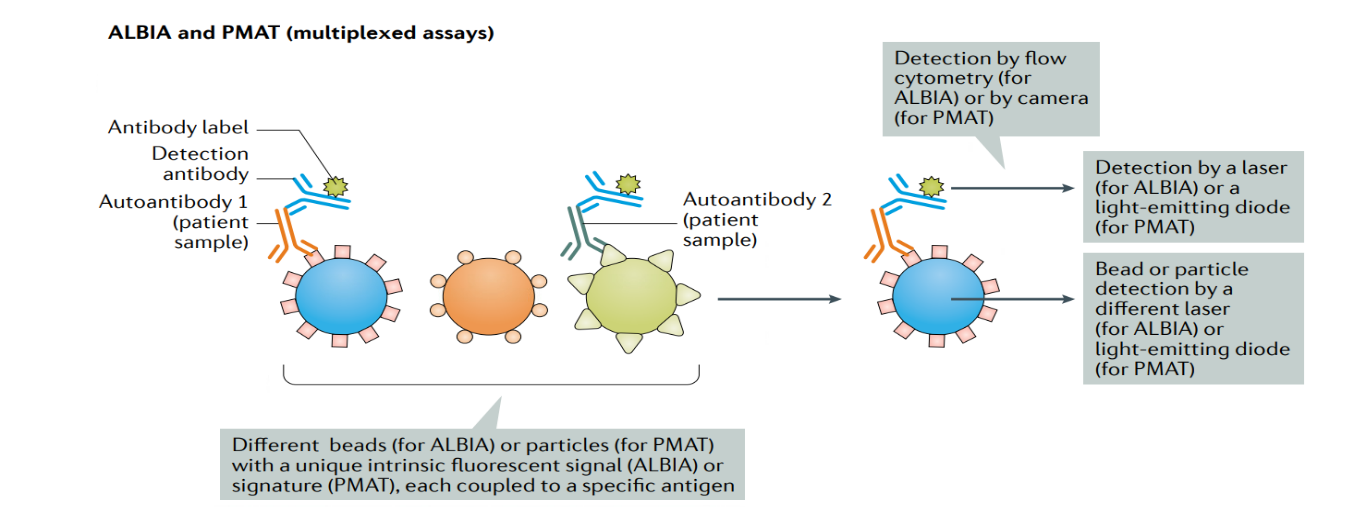
Newer Solid phase assays: ALBIA and PMAT